

Healthcare revenue cycle management isn't a billing department problem. It's a cash flow, compliance, and patient communication problem that shows up in billing first.
Most organizations already know how to submit claims. The harder issue is what happens between the first patient touchpoint and the final collected payment. That handoff breaks more often than leaders admit. Registration misses details. Eligibility isn't confirmed in time. Coding and billing move forward. Then the patient gets a confusing statement, the contact center has incomplete context, and collections turns into a slow, expensive recovery exercise.
The fix usually isn't another isolated billing tool. It's tighter control over the full payment journey, especially the point where billing turns into patient outreach and payment collection.
Healthcare revenue cycle management has become a major economic engine. The U.S. Revenue Cycle Management market reached USD 172.24 billion in 2024 and is projected to grow at a 10.1% CAGR from 2025 through 2030, according to Grand View Research's U.S. RCM market analysis.

That number matters because it changes the way leaders should view the function. RCM isn't a back-office utility anymore. It sits at the center of provider viability, especially when margins are tight, staffing is constrained, and every denied or delayed dollar has to be chased.
Most leaks don't start with a dramatic failure. They start with small operational misses that compound across the patient financial journey.
A registrar enters incomplete demographics. Insurance eligibility isn't verified before service. Coding has to work around weak documentation. The claim goes out late or wrong. The payer response creates more manual work. Then patient collections inherits a balance with poor notes, disconnected communication history, and limited payment context.
That's how organizations end up with three separate teams trying to solve one problem:
Practical rule: If patient communication and payment collection sit outside the core revenue workflow, revenue leakage will continue even when billing staff work harder.
The traditional split between billing and collections creates blind spots. Billing teams focus on adjudication. Contact center teams focus on outbound calls, inbound questions, and payment resolution. Patients experience the whole thing as one financial journey, but the organization often manages it as disconnected tasks.
That disconnect shows up in avoidable friction. A patient receives a statement, calls with a question, gets transferred, repeats account details, then leaves without paying. Nothing about that is a technology mystery. It's a workflow design problem.
A useful reality check comes from common collection breakdowns highlighted in this review of flaws in medical bill collections. The issue isn't just whether outreach happened. It's whether communication happened in the right sequence, with the right account context, and with a payment path that didn't create more friction.
Financial efficiency now carries the same operational weight as clinical throughput. Organizations that treat healthcare revenue cycle management as a strategic discipline tend to spot problems earlier. They look beyond claims submission and ask tougher questions.
Which balances stall after the first statement? Where do inbound payment calls drop? Which team owns the handoff from adjudicated claim to collected patient payment? Where does compliance risk increase because the communication stack and payment stack don't share controls?
Those are billing office questions now. They just don't stay in the billing office for long.
Healthcare revenue cycle management covers the full financial path from initial registration through final payment. That definition matters because leaders often shrink RCM down to claims and billing, then wonder why cash still gets trapped. The broader view is laid out in HFMA's overview of revenue cycle management, which also notes that effective RCM implementation can reduce days in A/R by 20–30% and lower denial rates by up to 40% when organizations enforce upfront eligibility checks and automated claim editing.
A healthier way to think about RCM is as a pipe with multiple joints. Money doesn't leak because one team failed in isolation. It leaks because each handoff depends on the last one being complete, accurate, and timely.
Registration hands data to eligibility. Eligibility hands coverage information to coding and billing. Billing hands balances and account status to payment posting, customer service, and patient collections. If one joint is loose, every downstream team spends time compensating for upstream defects.
That's why organizations can have competent staff and still struggle. The process itself forces rework.
Patients don't separate billing from collections. They experience one financial conversation with the provider. If that conversation starts with vague estimates, shifts into confusing statements, and ends in repetitive outreach with no easy payment path, the organization has an RCM problem even if the claim system is technically functioning.
A practical definition of healthcare revenue cycle management includes all of these moments:
The final payment isn't separate from revenue cycle management. It's the point where the whole process proves whether it worked.
Efforts often overemphasize pre-bill controls while underemphasizing post-bill execution. That creates a weak final mile. Claims may move through the system, but once a patient balance is created, ownership gets fuzzy. Billing says the statement was sent. The contact center says the patient couldn't authenticate quickly. Collections says the account lacked enough context to resolve objections. Finance sees aging balances grow.
That failure usually has three roots:
Strong healthcare revenue cycle management reduces avoidable friction at every handoff. That doesn't mean every balance gets paid immediately. It means the process is controlled.
A well-run cycle has clear ownership, clean data, reliable patient communication, and payment channels that match the way patients respond. It also treats every denial, inbound billing call, and broken payment promise as a process signal, not just a work queue.
When leaders define RCM this way, they stop asking only whether claims were submitted. They start asking whether the organization made it easy to get paid accurately, compliantly, and on time.
The revenue cycle breaks into three operational zones. Those are front-end, middle, and back-end processes. Kodiak Solutions' explanation of healthcare RCM stages notes that front-end failures such as inaccurate demographic entry or unverified insurance eligibility are responsible for approximately 60% of all claim denials.
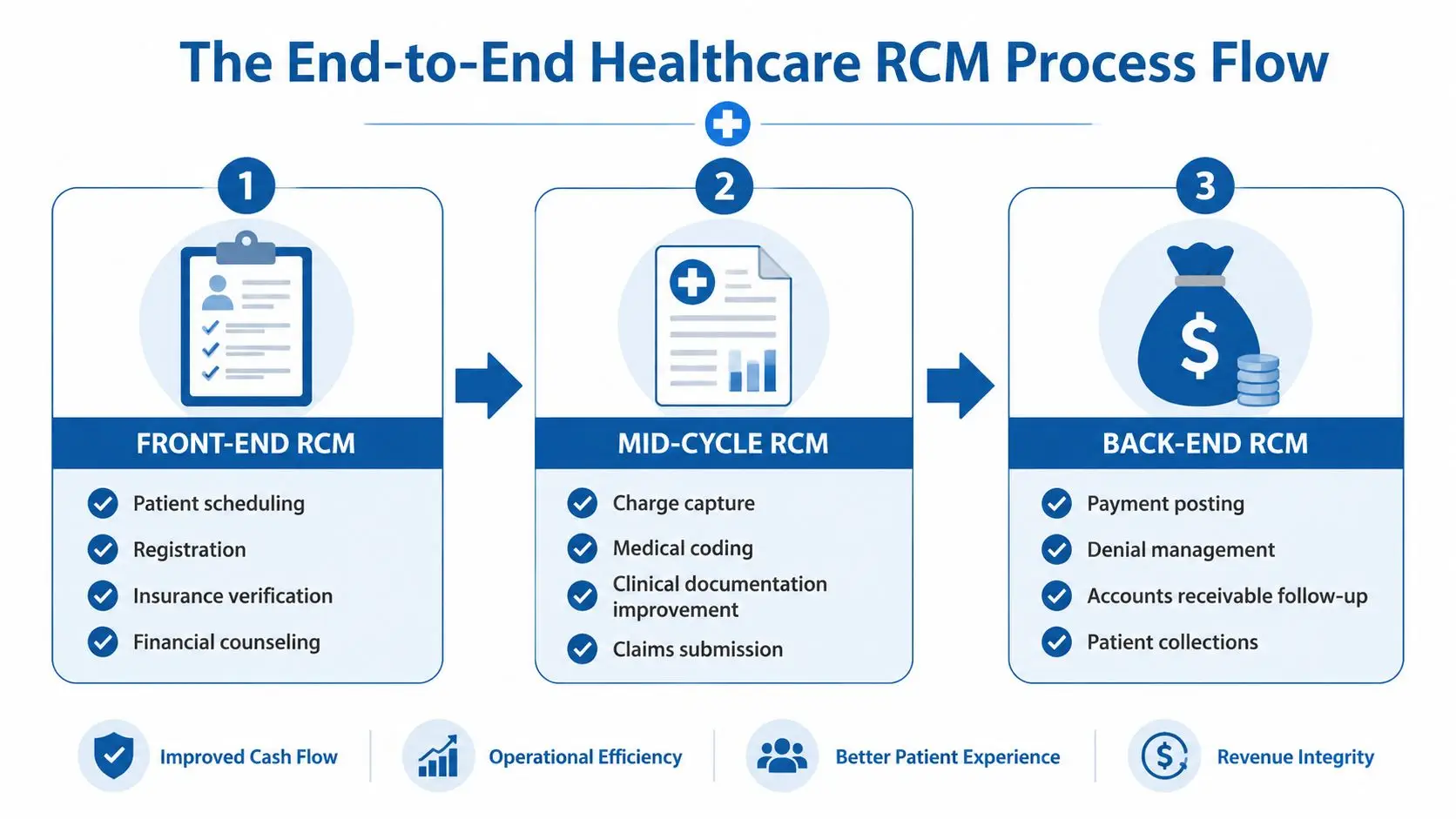
The front end determines whether the rest of the cycle has a chance, encompassing scheduling, registration, insurance verification, and financial counseling.
The goal is simple. Create a clean account before service. The common failure is also simple. Staff rush data capture, skip verification steps, or rely on stale insurance information.
Front-end work should focus on:
When this stage breaks, every downstream team pays for it.
The middle of the cycle translates care into billable, supportable claims. This includes documentation review, charge capture, coding, and claim generation.
Errors here often happen because clinical records don't support the code set, charges aren't entered on time, or coding teams have to interpret incomplete documentation. Even when the underlying care was appropriate, weak mid-cycle controls can create preventable denials and delayed submission.
A practical middle-cycle review asks:
| Process area | Primary objective | Common failure point |
|---|---|---|
| Documentation | Support the billed service | Missing detail or inconsistent notes |
| Charge capture | Record all services accurately | Late or incomplete charge entry |
| Coding | Align claim with clinical record | CPT and diagnosis mismatch |
| Claim creation | Produce a clean first submission | Edit failures ignored or overridden |
The back end decides whether booked revenue becomes collected cash. Its responsibilities include claim submission, denial management, payment posting, A/R follow-up, and patient collections.
Many organizations understate how much skill this stage requires. Posting payments correctly is one discipline. Working denials is another. Communicating with patients about balances, payment plans, and account resolution is another entirely.
Operational warning: A back-end team can't outwork a broken front end forever. It will spend its time recovering preventable errors instead of accelerating payment.
Three back-end failures show up repeatedly:
A single intake error can become four separate costs. It can trigger a denial, create rework, delay cash, and increase collection effort on the patient side. That's why process mapping matters. It shows where one miss becomes multiple labor events.
The strongest operating model treats every stage as connected. Front-end accuracy protects mid-cycle quality. Mid-cycle discipline protects payer reimbursement. Back-end coordination turns reimbursement activity and patient responsibility into actual cash without unnecessary friction.
RCM metrics should answer management questions, not just fill a dashboard. If a metric doesn't show where money is getting delayed, denied, or made harder to collect, it's not helping leadership.
The most useful scorecard combines claim quality, speed, and collection efficiency. One of the clearest benchmarks is cost to collect. Rivet Health's RCM metrics guide defines it as (Total RCM Costs / Total Collections) × 100, with industry averages for high-performing organizations ranging from 2.5% to 4.5%. The same source notes that improving clean claim rates to more than 95% can lower cost to collect by 1.5–2 percentage points.
These are the core metrics finance and revenue leaders should monitor consistently.
| Metric | What It Measures | Industry Benchmark |
|---|---|---|
| Cost to collect | Efficiency of total revenue cycle expense relative to collections | 2.5% to 4.5% for high-performing organizations |
| Clean claim rate | Percentage of claims submitted without errors that require rework | More than 95% |
| Days in A/R | Speed of converting billed revenue into cash | No benchmark cited in this section |
| Denial rate | Portion of claims that require correction, appeal, or write-off | No benchmark cited in this section |
| Patient collection yield | How effectively patient balances are converted into payment | No benchmark cited in this section |
Cost to collect answers whether the organization is spending too much to bring money in. If it rises, leadership should look at denial rework, call volume tied to confusing statements, manual posting exceptions, and fragmented collection workflows.
Clean claim rate is one of the clearest indicators of operational discipline. A poor result usually points back to front-end accuracy, coding edits, or weak claim scrubber rules. A stronger result reduces avoidable labor before the bill ever reaches a patient.
Days in A/R shows whether the cycle is moving or stalling. If that number drifts upward, the organization should separate payer delay from internal delay. Those are different problems and need different fixes.
Denial rate should never be viewed as a billing-only metric. Denials often expose registration errors, eligibility failures, coding mismatches, or missing authorizations.
Patient collection yield tells a different story than payer reimbursement. It reflects statement strategy, contact center effectiveness, payment options, self-service adoption, and whether the organization makes it easy to resolve a balance in one interaction.
“The biggest shift came when the team stopped treating denials, A/R, and patient payments as separate reports. Once they were managed as one operating system, decisions got faster and recovery got cleaner.”
A metric only matters if someone owns the response. Too many dashboards show a denial trend with no clear action path.
A better operating cadence looks like this:
The point isn't to collect more data. It's to make the next operational decision obvious.
Compliance failures in RCM usually happen during ordinary work. An agent answers a billing call, verifies the wrong fields, discusses too much account detail, takes a card payment, and leaves notes in a second system. Nothing about that interaction looks dramatic. It still creates risk.
That is why compliance belongs inside the operating workflow for communication and payment. In revenue cycle operations, the handoff between patient outreach and final payment is where controls often break. Billing may generate the balance correctly, but if the follow-up message, live conversation, and payment step do not follow the same rules, revenue and compliance both suffer.
HIPAA, TCPA, PCI-DSS, FDCPA, and FCRA all show up in day-to-day execution. They affect what staff can say, what systems can store, how outreach is triggered, and how payments are accepted.
The weak points are familiar:
None of these problems start in policy binders. They start in disconnected workflows.
A split RCM model makes compliance harder to sustain. One tool handles outbound reminders. Another stores notes. Another processes payments. Another records calls. Staff are left to bridge the gaps manually.
That manual handoff is where organizations lose control. An agent may need to switch screens to confirm consent status, then move again to take payment, then document the conversation somewhere else. Each extra step increases the chance of saying the wrong thing, capturing data in the wrong place, or missing an audit trail.
I have seen this pattern repeatedly. Teams train hard, monitor calls, and still get inconsistent results because the process itself asks staff to work across conflicting rules.
For organizations reviewing retention and handling standards in regulated environments, the Saskatchewan HIPA policy is a useful example of how operational design should follow policy requirements, not the other way around.
Secure outreach and secure payment should operate as one control framework. If the reminder is compliant but the payment step is not, the workflow failed. If the payment process is secure but the agent reveals protected information before verification, the workflow still failed.
A practical review should cover:
Teams tightening these controls can use this contact center security guidance for regulated communication environments as a practical reference.
They design the workflow so compliant behavior is the easiest behavior. That changes the result more than another annual policy review.
Agents should not have to guess what they can disclose. Supervisors should not have to reconcile outreach activity in one system with payment activity in another. Patients should not receive a compliant message that leads into a confusing or unsafe collection process.
Organizations that handle this well treat communication, documentation, and payment as one managed path. That reduces exposure, gives staff clearer rules, and closes one of the most common leaks in the revenue cycle: the gap between explaining the balance and collecting it.
A large share of patient balances never turns into cash because the handoff between billing communication and payment collection breaks down. That failure usually is not caused by a weak statement process or a weak collections team on its own. It happens because the patient gets one experience during billing and a different one during follow-up, with different systems, different records, and no shared workflow.
That gap is where revenue leaks.
RCM performs better when communication and payment live in the same operating path. Patients do not move through billing in neat stages. They open a statement, ignore a reminder, click a text link, call with a coverage question, ask for more time, then pay after work on their phone. If each step lands in a different system, staff lose context and patients lose confidence.
I see the same pattern in underperforming organizations. The billing office posts the balance correctly. The contact center reaches out. The patient finally responds. Then the agent cannot see prior messages, does not know whether a payment plan was offered, or has to send the patient somewhere else to complete payment. Collection effort goes up, resolution rates stay flat, and avoidable call volume climbs.
A unified workflow fixes that by connecting account status, outreach history, payment options, agent actions, and next steps in one place.
That improves performance in several places at once:
Automation only helps after the workflow stops breaking at the handoff. If the process is fragmented, automation sends more reminders, creates more tasks, and increases the volume of patient interactions that still end without payment.
The strongest use cases are practical and repetitive. Send the right reminder based on account status. Route callers by balance type or payment intent. Let patients resolve routine balances through self-service. Trigger follow-up after a missed promise to pay. Give agents one screen for communication, documentation, and payment capture instead of forcing them to swivel between tools.
The trade-off is straightforward. Highly customized workflows can mirror every department preference, but they often become harder to maintain and slower for front-line staff. Standardized workflows are easier to manage and train against, but they need enough flexibility for disputes, charity screening, hardship requests, and payment plans. Good RCM technology handles both without breaking the audit trail.
AI should reduce routine collection work, not create new compliance exposure. In healthcare, that means the AI has to operate inside the same controlled environment as the rest of the patient communication and payment process.
Grace is built as an AI collection agent for high-volume collection workflows. The value is not AI by itself. The value is that outreach, response handling, and payment activity stay connected inside a regulated communication and payment environment. That gives organizations a way to scale common collection interactions without adding the same amount of headcount.
Used correctly, collection AI can handle straightforward payment conversations, direct patients into self-service paths, and send exceptions to staff who need to resolve coverage questions or hardship requests. Used poorly, it creates one more disconnected layer between the patient question and the payment outcome.
A slow rollout protects the old leakage points. Healthcare finance teams rarely have the luxury to rebuild the entire revenue cycle before fixing billing communication and payment collection. The better approach is to connect outreach, agent workflow, and payment resolution to existing EHR, billing, and account data without forcing a major operational reset.
That is why workflow design matters more than a long feature list. If patients still have to jump channels to pay, or agents still have to leave the conversation to complete payment tasks, the workflow is still broken.
A useful test is simple. Can the organization move from outreach to verified account discussion to payment resolution in one continuous process? Teams assessing that model can review this unified contact center workflow for billing and payment operations as a practical reference.
RCM technology decisions show up in cash, patient experience, and audit exposure. Choose a partner that keeps communication and payment activity in one controlled workflow, and staff can resolve accounts faster with fewer handoffs. Choose a toolset that splits those steps apart, and the same leakage points stay in place.
That is the mistake I see most often. Leadership buys for features, while operations lives with gaps between the billing conversation and the payment outcome. In healthcare, that gap is where revenue slips. A patient gets a text, calls with a question, reaches an agent who cannot see the full account context, then gets pushed to another system to pay. Every extra step lowers completion rates and adds avoidable rework.
Start with workflow control, system design, and compliance discipline. Interface quality matters, but it does not fix broken handoffs.
A disciplined evaluation should cover:
Single-provider accountability
Ask whether the platform is built and managed by one provider or pieced together from third-party components. One owner usually means clearer responsibility, more consistent controls, and fewer support gaps when something breaks.
Connected communication and payment paths
Confirm that voice, SMS, email, chat, self-service payments, and agent-assisted payments operate in one process. If the patient has to leave the conversation to complete payment, the workflow is still leaking.
Concrete compliance controls
Ask how HIPAA, PCI-DSS, and TCPA requirements are enforced inside daily workflows. Look for audit trails, permission controls, authentication steps, and payment handling rules that work in practice, not just in policy documents.
Practical integration design
The partner should explain how account data, billing data, and conversation history flow into the agent view and payment workflow. Vague integration promises usually become delayed launches and manual workarounds.
Realistic implementation timeline
Long deployments often mean complexity the finance team will carry for months. Speed matters because unresolved communication and payment friction keeps draining collections performance.
Good evaluations get specific fast. A polished demo does not tell you what happens when a patient disputes a balance, asks for a payment option, or needs to authenticate before paying.
These questions surface the actual operating model:
| Evaluation area | What to ask |
|---|---|
| Workflow ownership | Who owns the full path from outreach to payment completion? |
| Compliance design | How are HIPAA, PCI-DSS, and TCPA controls enforced in daily agent workflows? |
| Integration | What data is required to go live, and how is account context surfaced to agents? |
| Reporting | Can reporting connect communication activity, payment behavior, and account outcomes? |
| Deployment | What is the realistic timeline to launch and what dependencies delay it? |
A regulated business needs a partner that understands how one workflow failure can create both cash loss and compliance risk.
Post-launch performance is the true test.
A strong partner helps the revenue cycle team improve scripts, routing logic, payment prompts, self-service use, and exception handling as account behavior changes. That support matters because patient communication and final payment are not separate operating problems. They are one collection workflow, and they need to be managed that way.
The payoff is practical. Agents spend less time switching systems. Supervisors get clearer visibility into outreach and payment results. Patients get a shorter path from question to resolution. Finance gets better control over the handoff where too many organizations still lose money.
Intelligent Contacts helps regulated organizations close the gap between patient communication and final payment. As a unified contact center and payments platform, it brings voice, SMS, email, chat, self-service payments, predictive dialing, routing, and secure payment processing into one workflow. Grace, the company's AI collection agent, supports compliant, high-volume collection operations. The platform is built in-house, integrates with existing systems, and is designed for fast implementation. For healthcare, ARM, financial services, insurance, government, utilities, and higher education teams that need one system for outreach and payment resolution, the next step is simple. Schedule a Demo or See Your ROI.














